
DynaMed® Medical Writer Amanda Thomason shares considerations for initiating insulin therapy in patients with type 2 diabetes. This is the third post in our series on insulin therapy for diabetes.
Type 2 Diabetes and Glycemic Control
Unlike patients with type 1 diabetes who must take life-long insulin because their bodies do not produce it, patients with type 2 diabetes typically start a medication regimen for glycemic control that includes oral agents such as Metformin.
Even when patients with type 2 diabetes require greater glucose lowering than can be achieved on oral agents alone, the American Diabetes Association (ADA) recommends that glucagon-like peptide 1 (GLP-1) receptor agonists be considered before insulin. In fact, expert organizations favor dual or triple non-insulin therapy as the initial treatment, and most clinicians would reserve starting insulin for patients only when specific indications manifest.
The bottom line regarding the choice of pharmacologic agents is to use a patient-centered approach that takes into consideration factors such as cardiovascular risk, hypoglycemia risk, effect on weight, cost, risk for adverse events, and patient preferences.
Indications for Insulin
The ADA suggests initiating insulin in patients with type 2 diabetes who have unplanned weight loss or other evidence of catabolism, symptomatic hyperglycemia (such as polyuria or polydipsia), or when HbA1c levels are above 10 percent or blood glucose levels are at or above 300 mg/dL (16.7 mmol/L). Moreover, when HbA1c levels reach at least 1.5 percent above the target in patients who have severe hyperglycemia and evidence of catabolism, insulin should be considered as part of any combination therapy to meet their goal HbA1c level.
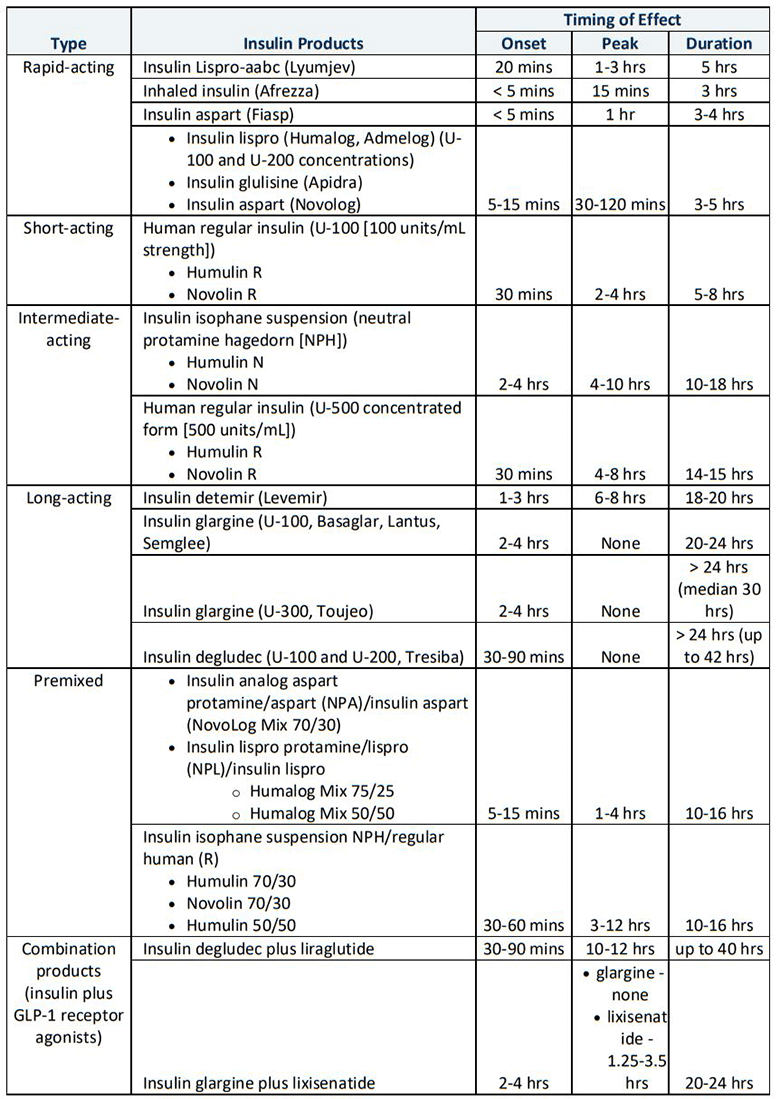
Types of Insulin
Insulin preparations range from rapid- to ultra-long-acting and include human and human analogs. The onset, peak and duration of action vary among types. The most common regular insulin and insulin analog concentration is 100 units/mL (U-100). However, more concentrated insulins exist (such as U-200 aspart and degludec, U-300 glargine, and U-500 regular), some of which have significantly different kinetics than the same medication at U-100 concentration. For example, U-300 glargine has lower hypoglycemia risk than U-100 glargine. The following table gives an overview of the various types of insulin available.
Insulin regimens for type 2 diabetes
In patients with type 2 diabetes, the preferred initial insulin is basal insulin. Options for basal insulin regimens include either a once daily administration of long-acting glargine (U-100 or U-300) or degludec (U-100 or U-200) or intermediate-acting NPH or intermediate-to-long-acting detemir insulin administered once or twice daily. A typical starting dose is 0.1–0.2 units/kg/day depending on the patient’s level of hyperglycemia, and the dosage is titrated as needed over days or weeks.
The addition of prandial (bolus) insulin to basal insulin may be necessary for patients with higher pretreatment HbA1c level, higher body mass index, longer duration of the disease, or greater number of oral glucose-lowering medications. Prandial insulin can improve overall glycemic control while allowing for flexible mealtimes and/or variations in diet. A reasonable initial dose is 10 percent the amount of basal insulin the patient is currently taking. It should be given before or with the largest meal or the meal with highest level of postprandial glucose excursion. The dose and number of injections can then be intensified based on prandial glucose excursions. Basal insulin intake may be lowered if the insulin regimen includes significant additions to prandial insulin, especially with the evening meal.
Inhaled insulin is an option for prandial insulin dosing, but spirometry testing is required before and after initiation of inhaled insulin therapy. Patients with chronic lung disease (such as asthma or chronic obstructive pulmonary disease) and who currently or recently smoke should not take inhaled insulin.
A basal-plus regimen may be used for insulin intensification in patients with type 2 diabetes in whom glycemic control is inadequate despite appropriate titration of basal insulin. This regimen may be an effective method to intensify insulin therapy prior to implementing a full basal-bolus regimen. In fact, a basal-plus regimen may be as effective and more practical than a full basal-bolus regimen if a simple, patient-directed titration algorithm is used that includes preprandial glucose targets and designates breakfast as the meal with which to administer the first prandial injection.
The use of an insulin pump is indicated for patients with type 2 diabetes who have marked insulin deficiency. Patients also use insulin pump calculators, which allow them to more easily calculate amount of nutritional insulin. The dose is based on the amount of carbohydrates in a meal plus the degree of preprandial hyperglycemia.
Premixed insulin formulations help provide some prandial insulin while limiting the number of injections required compared to basal-bolus or basal-plus regimens. However, premixed formulations may be more likely to cause hypoglycemia and/or weight gain compared to basal insulin alone, and patients cannot miss meals on premixed insulin without risking hypoglycemia. Premixed insulins offer both basal and bolus insulin coverage and are typically given twice daily, with two-thirds before breakfast and one-third before dinner. They may also be given as one daily dose before a large breakfast or dinner. Flexibility may be limited with premixed combinations to adjust dose, as both types of insulin in the mixture are adjusted concomitantly.
After starting insulin therapy, an evaluation of the medication regimen and medication-taking behavior is suggested every three to six months, with therapy adjusted as needed according to patient-specific factors that impact the choice of treatment.
For more information, see DynaMed topics in the Insulin Management suite, including Initiating Insulin in Type 1 and Type 2 Diabetes and Insulin Infusion Devices.


